

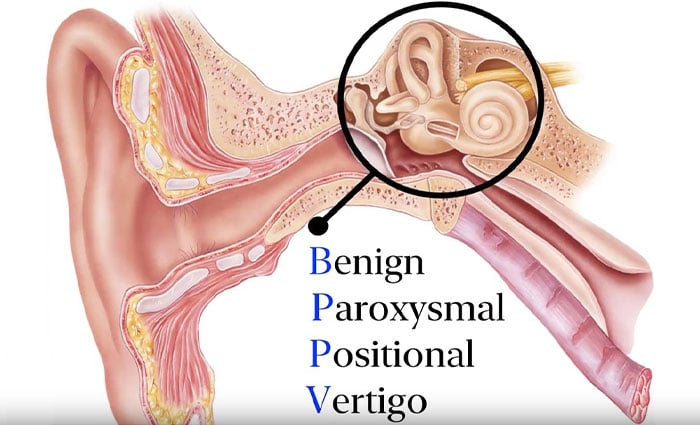
Benign positional vertigo (Benign paroxysmal positional vertigo -BPPV) is a disease that is characterized by dizziness and involuntary movements in the eyes (nystagmus) that occurs with certain head positions, and can usually resolve spontaneously over time.
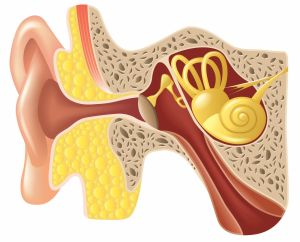
The cause of the disease is the escape of small calcium crystals (canallites) in the inner ear, which allow us to perceive gravity, to the balance channels opening to this region, following their release in the inner ear fluid, by breaking off from the region where they normally stay adhered, in the part of the inner ear called the vestibule.
Crystals escaping into the balance channel cause the nerve endings here to be stimulated after some head movements, resulting in typical complaints (canalithiasis). Although the shape and direction of the detected involuntary eye movements (nystagmus) vary according to the balance channel, in this disease, the posterior balance channel, which is usually in the lowest position relative to gravity, is involved, and the involvement of the horizontal and upper/anterior channels is extremely rare.
Before the mechanism of BPPV was clarified, various treatment methods were used in patients with this pathology. It has also been stated that avoiding head movements that trigger attacks is the most effective treatment method, since there is no effective drug treatment with proven benefits.
Today, in positional vertigo, “maneuvering therapy – canalith reposition”, which was first described by Epley and applied to remove the crystals from the channel where they escaped, is used for the treatment of complaints. CRM is the first treatment option to be preferred because the disease is self-limiting and can be controlled to a large extent with the canalith reposition maneuver (CRM) to remove the canaliths from the balance channels they enter.
Although the canalith reposition maneuver relieves the complaints related to the disease, it does not prevent the shedding of new crystals. For this reason, in order to prevent the recurrence of the disease, if there is an inner ear pathology such as Meniere's Disease that may cause crystal shedding by affecting the function of nerve cells in the inner ear, or if there is a systemic pathology such as circulatory disorder, diabetes, and thyroid gland dysfunction, this problem should also be treated.
There are also various surgical techniques defined to be applied in BPPV cases that do not respond to other treatment methods and affect the life of the patients.
Diagnosis of Positional Dizziness
In the patient's history, there is a feeling of dizziness that occurs with head movements and changes in body position,
Detection of involuntary eye movement (rotary nystagmus) with a rapid phase towards the lower ear that occurs after a waiting period of 2-5 seconds during the patient's head tilted backwards and hanging down (Dix-Hallpike test), and Simultaneous development of dizziness or nausea in the patient,
Short duration of nystagmus (usually less than 20 seconds)
Occurrence of nystagmus in the opposite direction and shorter duration when returning to a sitting position,
Exclusion of brain, brain stem, balance nerve and cerebellum pathologies by history, examination and, when necessary, hearing, balance tests and radiological evaluations.
Positional Dizziness Treatment
In most of the patients diagnosed with positional vertigo caused by crystal intrusion into the posterior balance canal, the complaints are relieved by the canalith reposition maneuver (CRM).
After CRM, patients are advised not to lie on the side of the diseased ear for 48 hours, to lie on their back or on the opposite side on a high pillow, not to lean forward, not to raise their head upwards, and to avoid sudden movements. Patients are called for control between 2 and 5 days, CRM is repeated in patients with nystagmus and or dizziness in the eyes with the control Dix-Hallpike test.
The rate of complete resolution of complaints with a single maneuver treatment is around 75-90%. With 2-3 treatments, 84 to 100% full recovery or a significant reduction in symptoms can be achieved.
Although the cause of positional vertigo cannot be fully found in most patients, the main causes that can be detected in some patients are; head traumas or concussions, advanced age, circulatory disorders, periods of sedentary bed rest and other ear diseases.
The high success rates show that maneuver therapy (CRM) is a painless and easy method as well as a highly effective treatment tool. Considering both the low rate of comorbidity and the successful results obtained with CRM, it is not necessary to apply standard diagnostic methods to distinguish other causes of dizziness in patients diagnosed with BPPV by the history and Dix-Hallpike test, thus providing an economical treatment. However, it is accepted that it is possible to avoid unnecessary and even uncomfortable advanced diagnostic methods.